Patient Responsibility For Non Covered Services Form - I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf. Service(s) not paid for by the benefit plan (practice name) accepts (plan.
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.

Fillable Online NONCOVERED SERVICES AGREEMENT Fax Email Print pdfFiller
I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf. Service(s) not paid for by the benefit plan (practice name) accepts (plan.
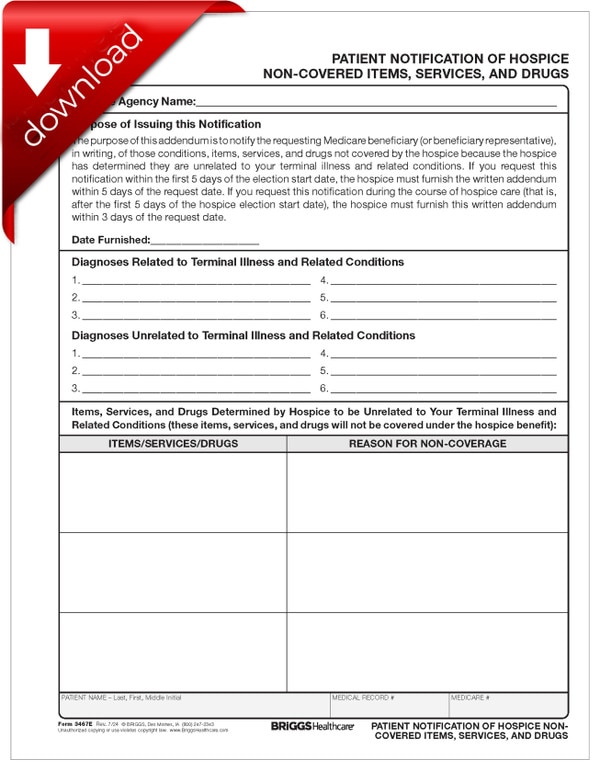
Patient Notification of Hospice NonCovered Items, Services, & Drugs
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.

Fillable Online Patient Billing Acknowledgement Form NonCovered
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
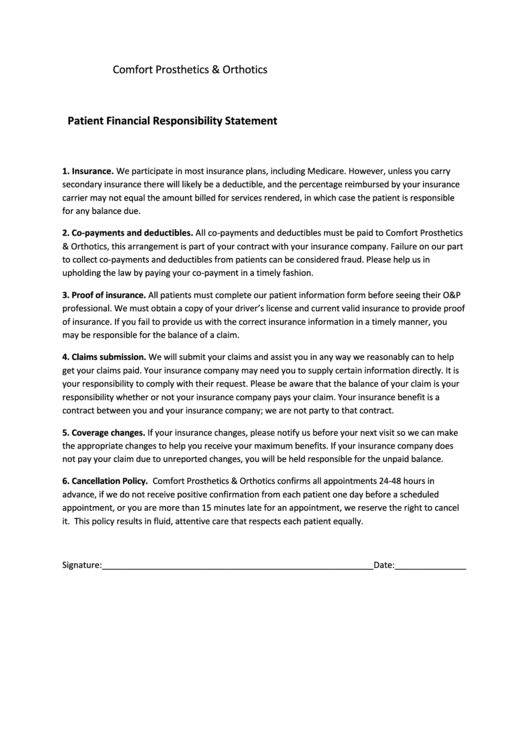
Top 8 Patient Financial Responsibility Form Templates free to download
I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf. Service(s) not paid for by the benefit plan (practice name) accepts (plan.

Patient Financial Responsibility Agreement Template PDF Template
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
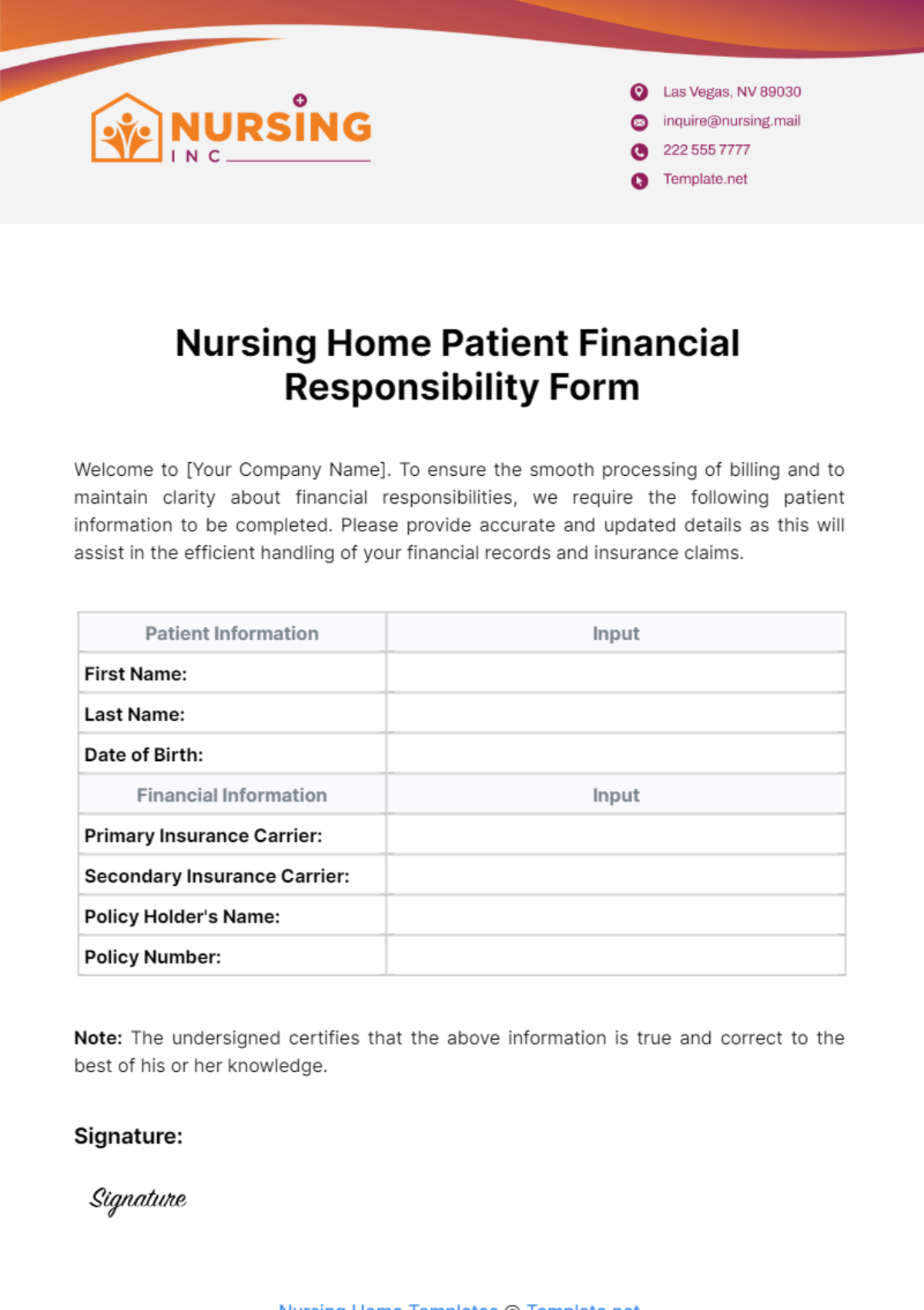
Nursing Home Patient Financial Responsibility Form Template Edit
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
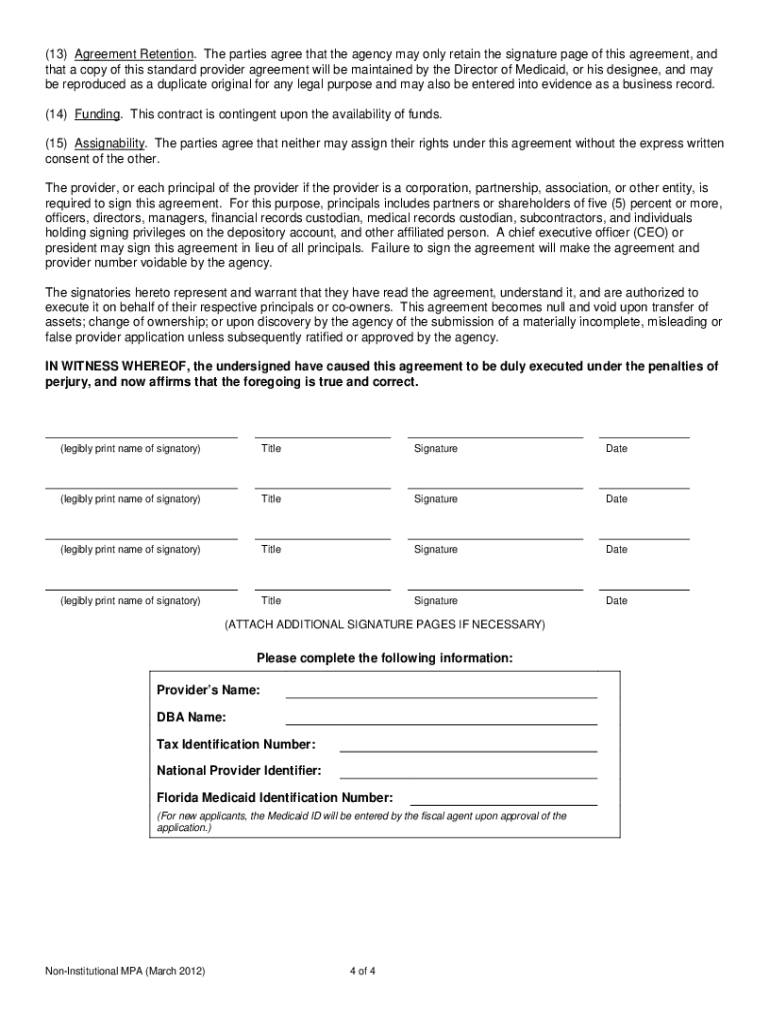
Medicaid Provider Agreement Non Institutional 20122025 Form Fill Out
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
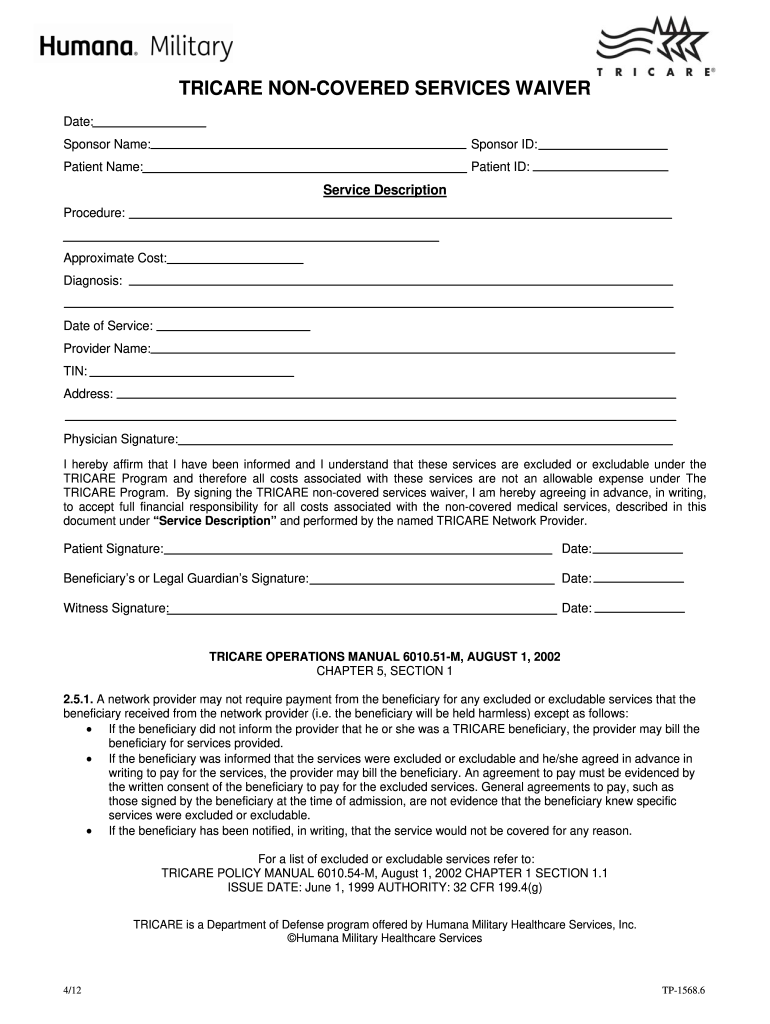
Trocar Non Covered Services Waiver Form Fill Out and Sign Printable
Service(s) not paid for by the benefit plan (practice name) accepts (plan. I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.
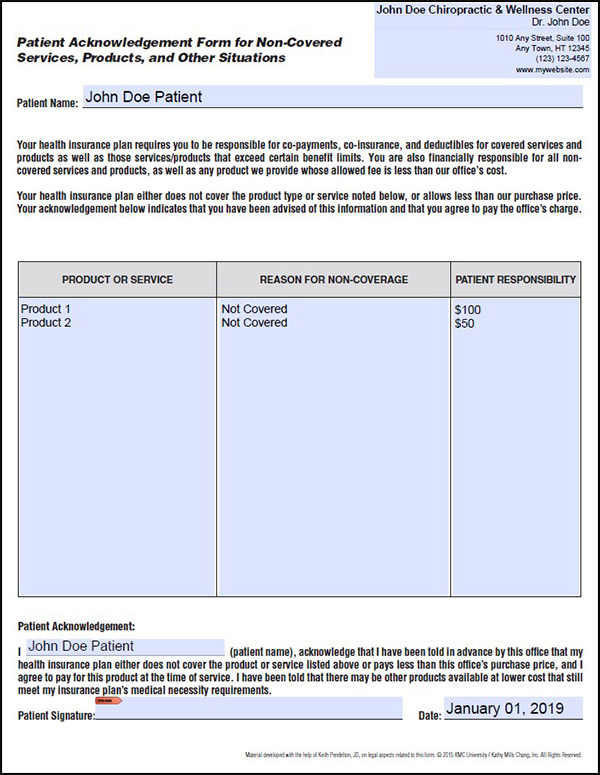
Patient Acknowledgement Form for NonCovered Services KMC University
I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf. Service(s) not paid for by the benefit plan (practice name) accepts (plan.
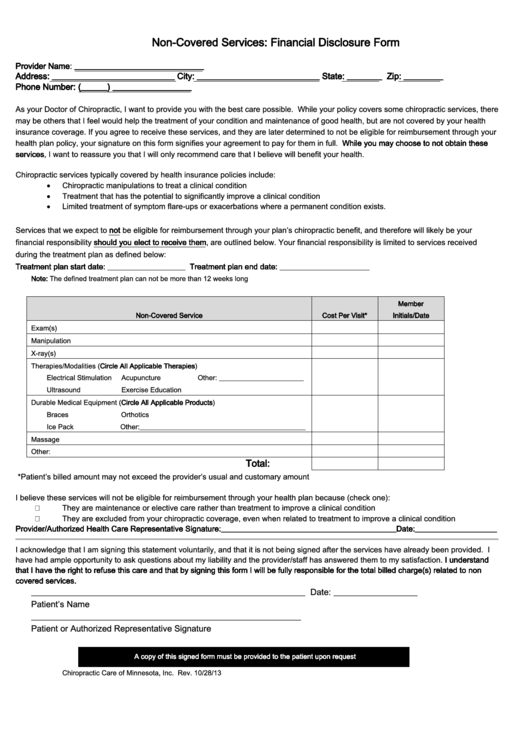
NonCovered Services Financial Disclosure Form 2013 printable pdf download
I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf. Service(s) not paid for by the benefit plan (practice name) accepts (plan.
Service(S) Not Paid For By The Benefit Plan (Practice Name) Accepts (Plan.
I request that payment of authorized medicare and/or medicaid benefits to me or on my behalf.